|
|

|
|
View in browser
|
Ribs, Anyone? New Chest Wall Injury Guidelines
02/24/2026
|
|
IT’S TRAUMA TUESDAY is
a Free Weekly Newsletter
Brought to you by
TCAR
Education Programs
|
|
For nurses and other clinicians
practicing anywhere
along the trauma care
spectrum
|
|
|
|
|
|
Take a quick test of your trauma care
knowledge
|

|

|

|
|
|
|
Article of the Week
To Fix or Not to Fix? Surgical Stabilization of Rib Fractures
|
|
|
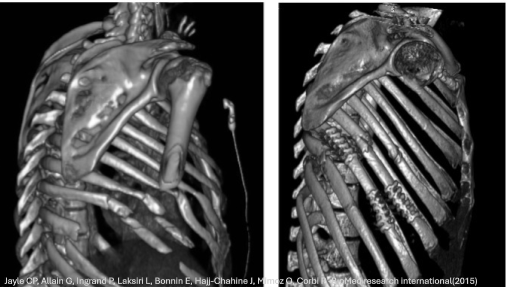
Well, there’s a Society for just about everything! The Chest Wall Injury Society has recently issued clinical guidelines for the surgical stabilization of rib fractures (SSRF). This document provides practical, evidence-based guidance on when operative rib fixation can meaningfully improve outcomes, including flail chest, significantly displaced rib fractures, and patients who can’t be weaned from the ventilator because the chest wall is too unstable or painful to support adequate breathing. The guidelines also outline situations when SSRF is NOT beneficial, such as for patients in shock and those with non-survivable brain injuries. For bedside trauma nurses, the key takeaway is that prompt recognition and escalation matter: the guidelines emphasize that earlier intervention (ideally within 72 hours) can shorten ventilator time and reduce pulmonary complications. This article supports RNs advocating for aggressive pain control, pulmonary hygiene, close monitoring for respiratory decline, and timely surgical consultation when rib fracture patients aren’t progressing as expected. Click the link to view the article or watch a short AI-generated article summary (7 min 59 sec).
|
|
|
|
Bauman ZM, Tian Y, Doben AR, et al. Chest Wall Injury Society guidelines for surgical stabilization of rib fractures: Indications, contraindications, and timing. Journal of Trauma and Acute Care Surgery. 9900:10.1097/TA.
|
|
|
|
Trauma Happenings
Do we Miss Hypotension Because of our Obsession with BP?
|

|
|
Does blood PRESSURE really matter? We routinely measure systolic and diastolic blood pressure, but these parameters are only surrogates for what we really want to know: Are the tissues perfused and oxygenated? Although a convenient measure that has been used for decades, BP has long been known to be a poor early predictor of end-organ perfusion. Changes in BP occur MUCH later than changes in perfusion, and it matters! Even short episodes of hypotension can have detrimental consequences for our patients. Check out this 7:40-minute video that explains the problem, its consequences, and the benefits of early detection.
|
|
|
|
|

|

|
|
TIC Talk in Austin
|
|
A personal invitation to all It’s Trauma Tuesday subscribers, Are you headed to Austin in April for the Society of Trauma Nurses TraumaCon? It’s not too late to register for this amazing annual event. This year, TCAR Education Programs’ very own Abbie Blackmore, MS RN TCRN, and Laura Criddle, PhD RN TCRN FAEN FAAN, will present TIC Talk, a fast-paced, interactive, case-based lecture focused on identifying and managing patients with trauma-induced coagulopathy, from field care to critical care. Join us at 0930 on Friday, April 17th. We’d love to meet you in person.
|
|
|
|
|

|
|
|
Speak Like a Pro
|
|
What do you call a minute, round, nonraised hemorrhage in the skin or in a mucous or serous membrane? It’s a petechiae. Sure, but can you pronounce it? This is one of those medical terms many people struggle to say, and the plural version is even harder, and there is rarely only one: One Petechiae. [pi-tee-kee-uh, or pi-tek-ee-uh]; Multiple Petechiae (puh-TEE-kee-ee or puh-TEE-kee-eye) The importance of these lesions varies depending on their cause. In severe sepsis, widespread inflammation, endothelial injury, and coagulation activation lead to disseminated intravascular coagulation (DIC), which results in petechiae formation. In a sepsis scenario, petechiae suggest septic shock and multiorgan failure. In trauma, petechiae are often associated with traumatic asphyxia- a sudden severe compression of the chest or upper abdomen while the glottis is closed (e.g., MVC, crush injuries, heavy object compression). This leads to capillary rupture and the extravasation of blood into the skin and mucosa, resulting in petechiae on the face and upper chest. Facial petechiae in pediatric trauma patients are a sentinel finding, as this clinical sign is rare in accidental childhood injuries. Abuse-related mechanisms associated with facial petechiae include manual strangulation, suffocation, smothering, chest compression, or being forcibly held face-down. Be prepared to make appropriate referrals. Click the link to hear it pronounced on the Dictionary.com site!
|
|
|
|
|

|
|
|
|
|
|
Follow Us
Want to join the trauma care conversation?
Follow Us on Facebook, Instagram, and X.
|

|
|
|
|
|

|
|
TCAR
Education Programs
tcarprograms.org
info@tcarprograms.org
Office: (503) 608-4900
International Toll-Free: +1 800-800-2015
|
|
|
|
Copyright © 2026 TCAR Education Programs. All rights reserved.
You are receiving this email because you opted in by purchasing or registering for a
course or subscribing to our newsletter on our website.
Want to change how you receive these emails?
You can
update
your preferences or
unsubscribe
|
|
|